A 39 year Chinese man with locally advanced rectal cancer. Mr Chia first presented with difficulty in motion in Jan 2005. He was then in severe pain and had bleeding whenever he went to the toilet. He also passed motion with difficulty and pain. Clinical examination showed a huge rectal mass fixed to the pelvis and protruding into the anal canal. The lower end of the cancer was only 2 cm from the bottom of the anus. He saw a surgeon elsewhere and he was advised that no treatment was possible and that he should go home and await the end.
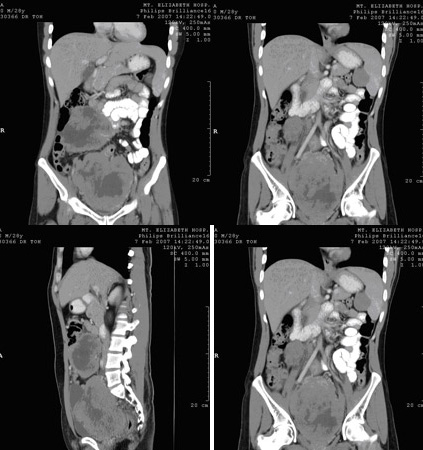
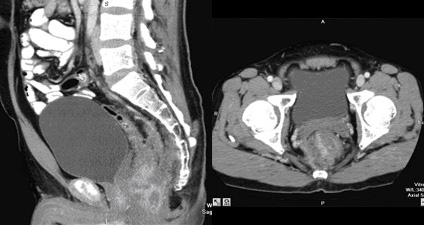
Mr Chia became desperate until a friend recommended him to see me at Mt Elizabeth Hospital. Clinical examination showed Mr Chia to be a well built man in his late 30’s. He was fit and physical examination showed no abnormality except for the huge fixed cancer in the pelvis and rectum. CT films showed gross infiltration outside the rectum and a huge mass was immediately clearly seen. The cancer was clearly not completely respectable at this stage. He was advised to undergo chemotherapy and radiotherapy in an effort to shrink the cancer. This strategy worked well.
Six weeks of chemo and radiotherapy shrunk the mass completely. After 6 weeks, no residual cancer was felt on rectal examination. Further X rays showed spread elsewhere and Mr Chia was advised for rectal surgery. An ultra-low anterior resection was done on Oct 2006. Histological examination of the resected specimen showed complete clearance of cancer. Mr Chia is expected to have a good prognosis.